
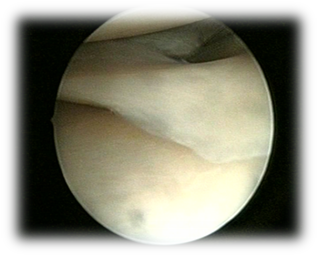
The knee joint has two menisci, the medial and the lateral. They act like cushions between the femoral and the tibial bone. They consist of collagen and proteoglycans, and are specially shaped so that they bring together two non-matching articular surfaces. They also contribute significantly to joint stability, joint motion, while also protecting the cartilage, thus preventing osteoarthritis.
Meniscus has blood vessels only in its peripheral 25%, that derive from the synovial membrane and joint capsule. The central 75% of the meniscus has no vessels, and gets its nutrition from the joint fluid. This is the reason that only peripheral tears of the menisci located in the so-called red-red zone can heal with conservative treatment.

Central lesions do not heal, and can deteriorate with activities, leading to cartilage lesions. Knee function becomes problematic, and sports activities are limited.
Up to the 1980s open total meniscectomy was used for treatment of meniscal tears – a procedure that caused great damage to the knee and required a long rehabilitation period. Long-term follow-up of these patients also revealed that osteoarthritis developed in all these patients that the meniscus had been removed within 3 years post-operatively.
The need to minimize the trauma in the knee led to knee arthroscopy. With the use of a tiny camera that inserts the knee through a very small skin incision, the knee joint is scoped, the lesion is identified, and the tear of the meniscus can be treated either by suturing it or by excising only the torn part of it, thus leaving the rest of the meniscus intact. This partial meniscectomy proved to be a safe method with a great outcome in the long-term. However, in high-demand young athletes, the only solution to anatomically restore the knee anatomy is meniscal repair with sutures.
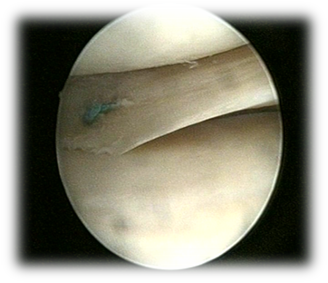
Unfortunately, meniscal repair can only be performed in the red-red zone of the meniscus, because this is the only area where healing can be expected.
In cases of tears of the whole meniscus synthetic or cadaveric meniscal grafts can be used, and arthroscopic meniscal transplantation can be a solution.
Lately, new minimal invasive meniscal repair methods have been developed (all inside repair) that are highly efficient, with low complication rate and cost. According to literature, the failure rate of this type of repair is 9-18%, depending on the size of the tear, the time form injury to the repair, the location of the tear in the red-red or red-white zone, as well as the presence of associated lesions in the knee (eg. anterior cruciate ligament tear). In our hands, repair of the meniscus is successful in more than 80% of the cases.

In doubtful cases, given the importance of maintaining as much meniscal tissue as possible, it is preferable to risk repairing the meniscus than go for a meniscectomy.
Rehabilitation following meniscal repair is 2 to 3 months longer than that following meniscectomy, but the outcome is worthwhile.
Surgical intervention for meniscal tears is necessary in most cases. The modern techniques of meniscal repair or meniscus transplantation when necessary, have revolutionized the efforts to prevent knee osteoarthritis.
The TheMIS orthopaedic team has great experience in the treatment of meniscal tears using all the latest methods available (partial meniscectomy, menisal repair with all inside, inside out, outside in techniques, meniscus transplantation). Additionally, TheMIS Orthopaedic Center is part of Smartsurg, a European scientific program funded by the European Union, that plans to create a robotic arm to perform arthroscopic meniscectomy or meniscal repair.